

This article provides an in-depth look at knock knees and bow legs — two common leg-alignment conditions in children. Although they are opposite deformities, they share many of the same causes, the same diagnostic workup, and the same treatment options. This guide explains both, so parents in Delhi can recognise the condition early and seek the right care.
Knock Knees (Genu Valgum)
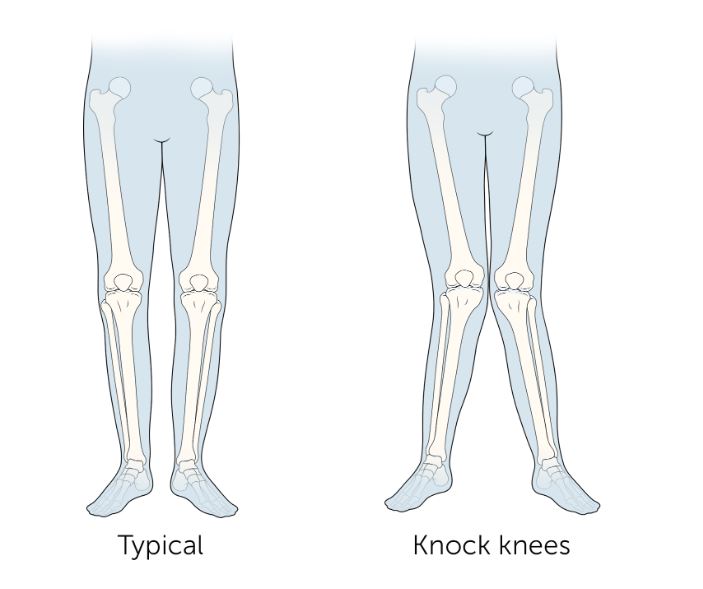
Knock knees is a condition in which the knees angle inward and touch each other when a person stands straight, while the ankles remain apart. This condition is medically known as genu valgum. It is commonly seen in children and is often a normal part of growth and development — in most cases, the alignment corrects itself naturally as the child grows. However, in some individuals, knock knees may persist into adolescence or adulthood, leading to pain, difficulty in walking, early joint wear, and functional limitations.
Bow Legs (Genu Varum)
Bow legs is the opposite condition — one or both legs curve outward at the knees, creating a wider-than-normal space between the knees and lower legs. When the child stands with feet and ankles together, the knees stay wide apart, giving a bow-like appearance, especially while walking. Medically called genu varum, bow legs are very common in infants and toddlers and rarely serious — babies typically outgrow it by around 18 months. If it persists in older children, evaluation by a specialist is important.
Normal Leg Development in Children
The development of leg alignment in children follows a predictable pattern. Infants commonly have bow legs until about 2 years of age. Between 2 and 3 years, the legs often shift into a knock-knee alignment. By around 7 years of age, the legs usually straighten into a normal adult alignment.
In most children, these phases are temporary and normal. Persistent or worsening deformity beyond these ages may require further evaluation.
Benefits of Early Intervention
Early intervention can prevent the need for more invasive procedures later. Addressing the condition while the growth plates are still open allows for simpler corrective measures — such as growth modulation, a minor procedure that gently guides the natural growth of the bones back into alignment without major surgery.
Symptoms
Knock Knees
- Visible inward angulation of the knees when standing
- Knees touching or nearly touching with feet apart
- Difficulty in walking or running
- Knee pain or discomfort, especially after activity
- Uneven shoe wear or associated foot pain
- In some children, facial structure changes associated with underlying vitamin D deficiency
Bow Legs
- Outward bowing of the knees, with the lower legs angled away from each other
- Persisting beyond the age of 2–3
- The angle of the thigh bone falling outside the normal range
- Mismatch between the direction of the foot and the direction of the knees
- One leg appearing more bent or curved than the other
Causes and Risk Factors
Both knock knees and bow legs share many of the same underlying causes. Vitamin D deficiency, which is crucial for bone health and development, is a leading cause — it can lead to rickets, a condition that softens the bones and causes deformities. Reduced sunlight exposure, noted particularly during the COVID-19 pandemic, has increased cases due to lower vitamin D synthesis.
Other contributing factors include:
- Normal growth and development in early childhood (often self-correcting)
- Abnormal bone development or metabolic disorders
- Obesity, which increases stress on the knee joints
- Ligament laxity or muscle imbalance around the knee
- Previous injury affecting bone alignment
- Blount’s disease (bow legs specific) — a growth-plate disorder of the shin bone, more common in children who are overweight or walk early
- Dwarfism caused by achondroplasia (can produce bow legs)
- Fractures that haven’t healed completely or abnormally developed bones
- Fluoride or lead poisoning
Diagnosis
Diagnosis begins with a detailed clinical examination, including assessment of leg alignment and gait. A thorough medical and family history is also taken. In children under 2 with mild bow legs, no further testing may be needed — the deformity is usually a normal phase of development.
When the deformity is persistent or severe, a standing alignment X-ray or EOS scan is performed. This imaging captures the entire limb from hip to ankle and helps determine the mechanical axis and the exact location of the deformity, allowing the orthopaedic surgeon to plan appropriate treatment. Blood tests may be ordered to check for vitamin D, calcium, or metabolic causes.
Treatment Options
Treatment depends on the age of the child, the severity, and whether the growth plates are still open.
Non-Surgical Care
- Observation, as many cases resolve naturally with growth
- Vitamin D and calcium supplementation when deficiency is the underlying cause
- Physiotherapy to improve strength, alignment, and joint support
- Bracing or orthotics — particularly used for early-stage bow legs to gradually pull the legs into a straighter position over time
- Weight management through a healthy lifestyle
Growth Modulation (Hemiepiphysiodesis — for children with open growth plates)
A minor, reversible procedure with minimal blood loss. A small clip is placed on one side of the growth plate to temporarily arrest growth there, while the other side continues to grow — gently correcting the deformity over 6–12 months. This is the preferred surgical approach when the growth plates are still open.
Gradual Correction Using External Fixators
Recommended for select children under 10 with significant deformity. The surgeon cuts the bone and applies an adjustable external frame using wires and pins. The frame can be fine-tuned during the day-to-day, and the child can continue daily activities. Regular follow-ups monitor healing progress.
Osteotomy (for older patients with closed growth plates)
Once the growth plates have closed, growth modulation is no longer an option. In these cases, an osteotomy may be needed — the bone is cut and realigned, then stabilised with a plate and screws. Acute correction takes 6–8 weeks of careful immobilisation to allow proper healing.
Recovery and What to Expect
Recovery from growth modulation is relatively quick — children often resume normal activities shortly after, with gradual correction over months as the bone grows. External fixator treatment allows daily activity during correction, with follow-ups to adjust the frame. Osteotomy requires a longer recovery during which weight-bearing is limited; the child may need a walker or crutches for a few weeks. Across all approaches, physiotherapy is central to restoring strength, mobility, and gait.
General timelines range from 6 weeks to several months depending on the procedure and severity. Regular follow-up with the surgeon ensures the bone is healing correctly and the alignment is on track.
Cost of Knock Knees & Bow Legs Treatment in Delhi
The average cost of corrective treatment in Delhi typically starts from ₹6,00,000 and can reach up to ₹8,00,000 for complex surgical correction. Several factors influence the final cost:
- High-end private clinics with specialised paediatric orthopaedic facilities charge more than standard hospitals.
- The severity of the condition — advanced cases require more complex procedures.
- The experience and expertise of the surgeon.
- Pre-surgical tests, including X-rays and advanced imaging.
- Length of hospital stay and post-surgical care requirements.
Why Choose Dr. Ashwani Maichand
With three decades of experience in orthopaedics, Dr. Ashwani Maichand specialises in advanced corrective techniques for children — including deformity correction, guided growth, external fixator application (including Ilizarov and hexapod frames), and osteotomy. Treatment is tailored to each child’s age, growth status, and severity of deformity.
With his patient-centric approach, Dr. Maichand focuses on early diagnosis, precise correction, and long-term functional outcomes — ensuring minimal discomfort, quick recovery, and improved limb alignment of the child.
FAQs
Conclusion
Understanding and addressing knock knees or bow legs early is crucial for effective treatment and for preventing the need for more invasive procedures later. For expert evaluation and personalised treatment, consult Dr. Ashwani Maichand at Minomax Orthopaedics in Delhi.
Patient Stories and Videos